12 Bere 2024
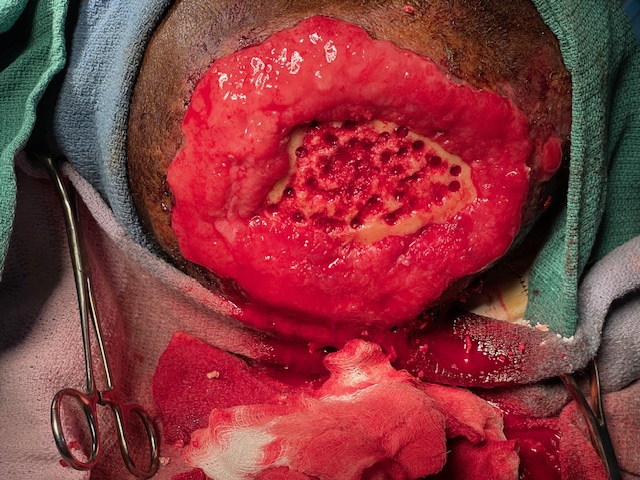
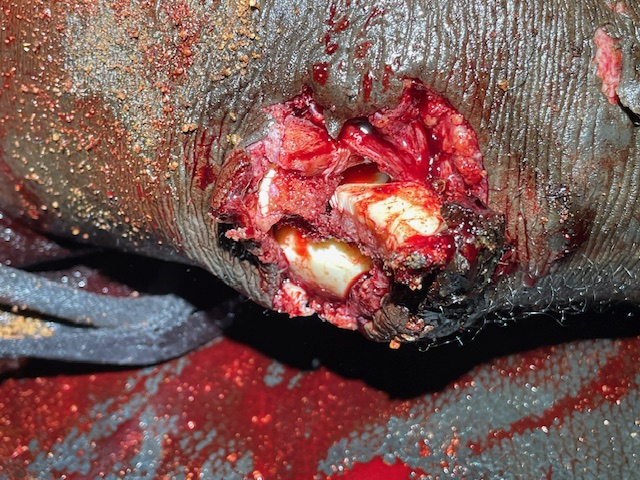
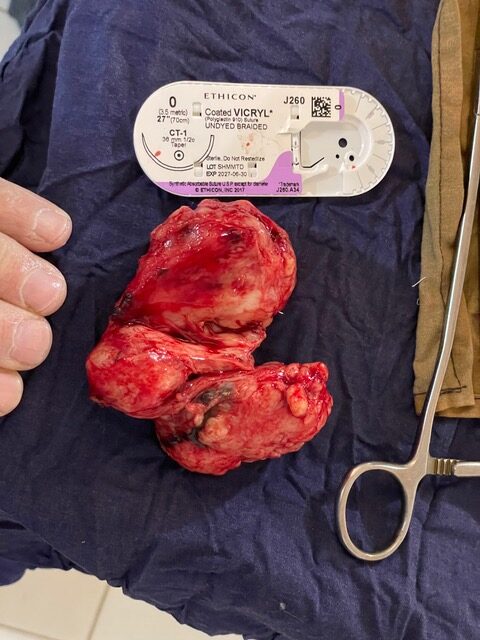
It’s my last day in Bere and we have planned a long day, and it just gets LONGER!! I start with a number of scheduled cases then have to cancel some scheduled to accommodate emergency after emergency. I realize it’s Friday and there are no meetings so i go in earlier about 7:30. I find Phillipe in the OR and ask him when i can start. He said the kid with the cheek abscess is ready and we should do him early so that he can eat. So I tell him to put him to sleep and Ill get ready. he gives him a little Propofol and I lance his cheek and get nothing. It felt fluctuant and the dad said pus had been draining out of two small holes. I go deep and get nothing. So I probe the holes and they are real superficial. So I biopsy a large lymph node near by and then close back up the hole I made, suturing it shut.
I run over to the surgical ward and tell the nurse, Emma, Ill try to round with him later, but to go ahead and do dressings… and let me know if there are problems. He says the emaciated woman that Ive been watching and I wrote about in 11 Bere 2024, is nauseous, so I decide to give her metoclopramide to see if stimulating her bowels will resolve her issues. Later she’s vomiting and then I chose to operate on her like i previously mentioned in the last Shanksteps.. So that was an emergency later in the day. So after talking to him I continue operating.
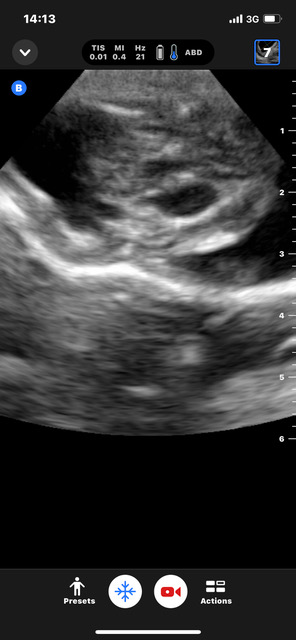
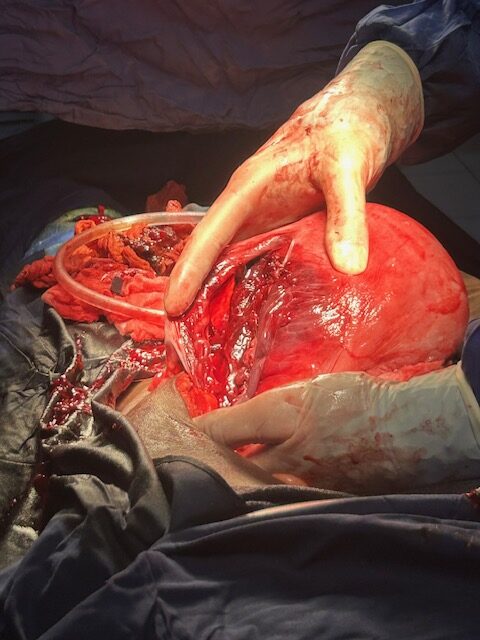
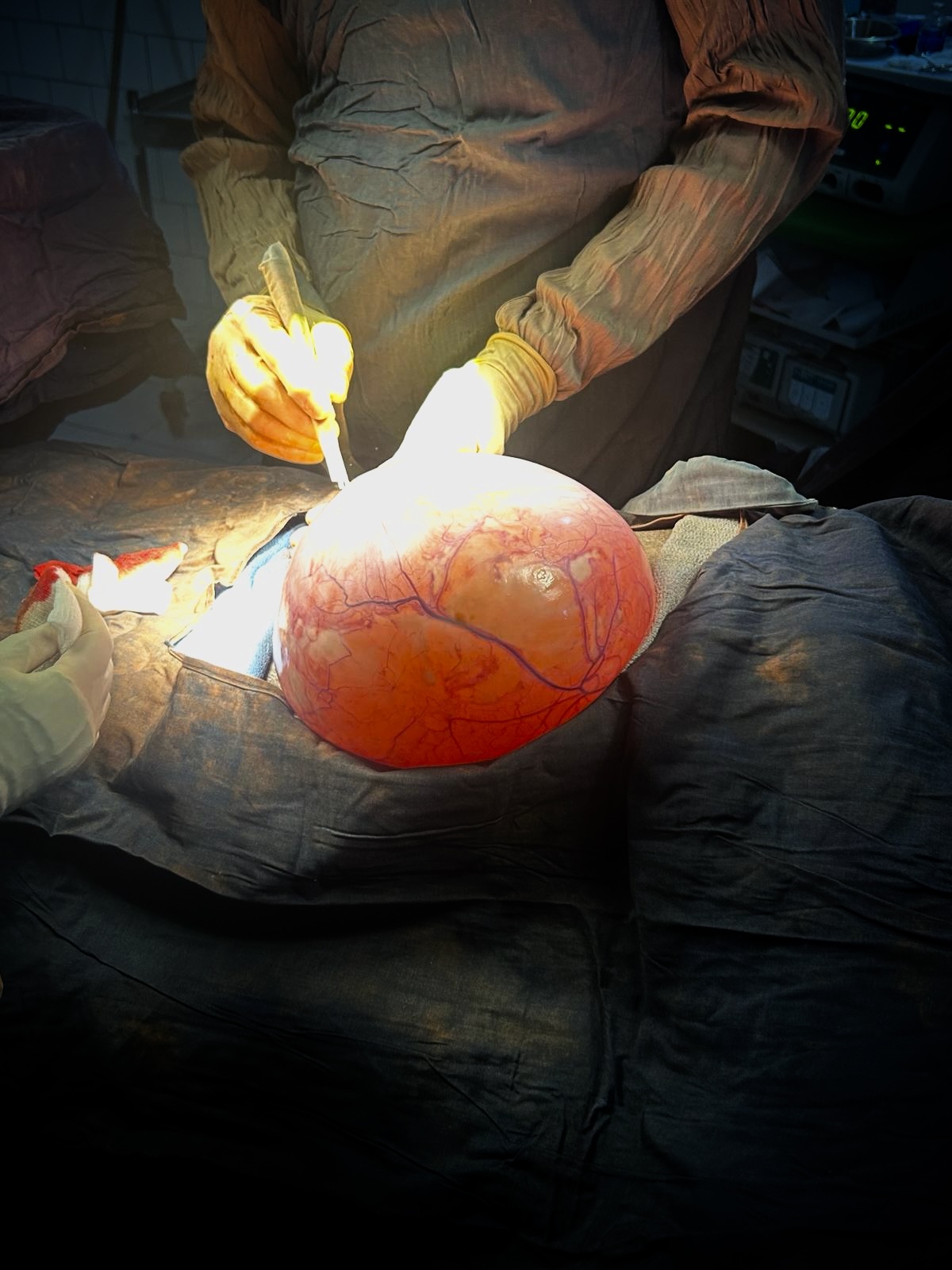
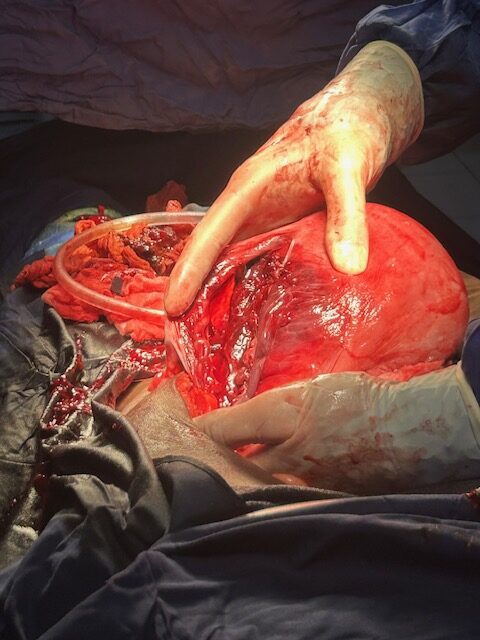
A woman is brought from the emergency room who has an ectopic pregnancy- one that is outside the uterus. She has the ultrasound report that says so. I ultrasound her and think I see a rib cage outside the uterus. I don’t really see all the normal features of a fetus so I ask Audrey to come take a look. So she comes over from maternity. She looks around and doesn’t find anything but an irregular looking mass outside the uterus that has the appearance of a uterine fibroid. We’ve heard of pedunculated fibroids that can hang off the uterus, so assume it may be that. The patient has a negative pregnancy test which goes against an ectopic pregnancy. She says she has been pregnant 14 months and the baby hasn’t moved the past 4 months. I open up her abdomen and do not find a abdomen full of blood as is common with presentation of an ectopic. I find the omentum stuck to a large mass. slowly I free up the omentum from the mass. Then as I free up more from behind the mass I see a hand. Oh this IS a ectopic pregnancy. As i identify more I find there is a fetus wrapped in omentum. It’s head is not fully formed, I think if may be anencephalic. So after getting it out there remained a mass further in the pelvis. I free this up and it’s the placenta. The baby was near term and was fed by blood from the omentum. I’ve read about this being a possibility in the books, but I’ve never seen one. Very strange!
The next two operations of the day were the two that I discussed in 11 Bere 2024. One was the intestinal blockage after surgery somewhere else, and the second was a perforation of intestine of a boy after falling on the handlebar of his bicycle.
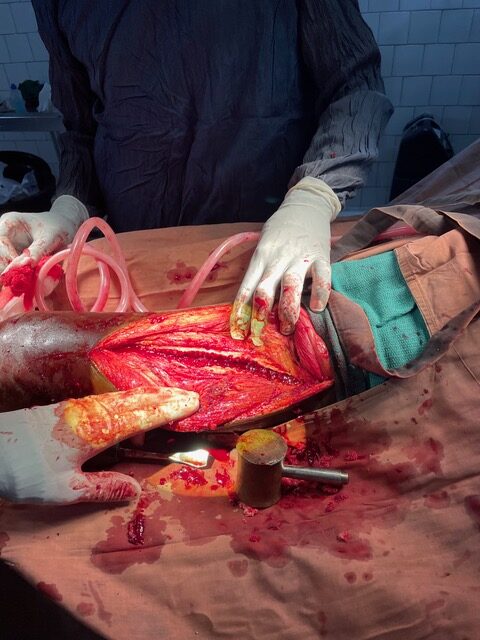
Next was a guy that the ER had sent over. When you think of ER you think of a room glowing with light and different patient rooms and doctors and nurses running around taking care of emergencies left and right. They’re calling other doctors to come and admit patients to different services in the hospital after getting lab work, CT scans, and X-rays. Am i right? The ER here is a nurse with two or three nursing students who jot down the patients complaints in the patient’s little medical booklet they keep with them, or they lose it and get a new one when they arrive. Then the nurse decides what tests to get and what lab-work seems appropriate to them. So this guy comes in with a huge scrotum that is painful and he has had a hernia a long time. So the nurse orders a glucose test, malaria test, typhoid test, and sends him to the OR to be evaluated by us. Well the last one was the appropriate one. He has a large hernia that makes his scrotum look like a small watermelon. I’m unable to reduce it (push it back inside). So he’s next in the OR. He gets a spinal anesthetic and then I open his groin. I start opening the different layers and it still doesn’t reduce. Finally I open the hernia sac and see colon in it. The colon is viable and so I slowly push it back inside. Once the sac is empty, I separate it from the surrounding structures and then cut it off keeping clamps on the opening. I then close the sac. Then I do a tissue repair called a modified Bassini. Closing the native tissues over the hole. i don’t use mesh here for two reasons. We don’t have much and secondly I still worry about wound infections and therefore mesh infections. It doesn’t seem like there are many recurrences here, and I think part of the reason is that there are no narcotic pain medications, so people feel when they are pulling on the repair and don’t do things they shouldn’t. We get done and I see that last of the consults that are waiting and then head back to our room. It’s about 9 PM and I pray that we will have a calm night. we plan to leave at 7 AM and I don’t want to do an emergency especially around 7AM when we need to leave and the other doctors aren’t quite back yet.
We sleep for an hour or two and are called by the maternity nurse for a delivering mother who has vaginal bleeding. Audrey heads in and I know we will have to operate on her so I head in shortly there after. Audrey is already headed back to get me. She says there is blood everywhere and the baby is still alive. I call Phillipe and David (anesthetist and circulator). I see the patient in the bed of the delivery room. (The delivery room is a room with 5 beds lined up against one wall. If there are multiple women in labor they lie on the beds all lined up as they suffer. The nurse may catch one after another like has happened many times.). So back to the woman at hand- she is absolutely covered in blood all over her cloths and there is a widening 4 foot pool of blood on the floor. WOW!!!! That’s a lot of blood. I run to the OR and get out two units of blood of her type and stick one under each armpit to start warming them. I also grab a couple saline bags and run back to maternity. I ask the nursing students to get the gurney from the OR and start wheeling her over there. The nurse is getting in another IV line. I also grabbed the transfusion tubing. We start pouring in the fluids. And we get her headed to the OR. We get her laying on the OR table and stick in the second IV and get the anesthesia monitors connected. Phillipe and David make it in and the blood is warmed up and Phillipe starts it as I get the OR kit for the C-section ready. I get the gloves and suture and gauze…all opened on the scrub table. Phillipe gives her a whiff of Ketamine and I open. She groans a little but will have no recollection of it. I go in all with a scalpel as fast as possible. Through the abdomen and then into the uterus. I pull out the baby and we hand it off to David. I scoop out the placenta and start closing the uterus. I didn’t take the time to find out why she was bleeding, just took care of the placenta so it would stop. I ask David how it’s going as Im not hearing the baby cry. I ask if he wants help and he does. So Audrey scrubs out helps give the baby CPR. Giving breaths and oxygen and chest compressions. It takes a couple minutes before the baby’s heart started and started to breath. She never really cried but moving extremities. I close the uterus as best I can by myself and finally David scrubs in to help me. Mom is doing well with three units of blood and baby is alive. We leave as they start to mop up all the blood all around. We are grateful to have a last live mom and baby for this trip!! We sleep for a few hours then get up to start our three day trip home.





















 I want God to use me like he did David Wilkerson. Not for kids in NY but however He sees fit.
I want God to use me like he did David Wilkerson. Not for kids in NY but however He sees fit.